State Licensing Boards, Antitrust, and Innovation

In this paper, James Cooper, Elyse Dorsey, and Joshua Wright discuss occupational licensing boards, competition, and the role antitrust law can play in the marketplace.
Contributors
James C. Cooper
Elyse Dorsey
Joshua D. Wright
This paper was the work of multiple authors. No assumption should be made that any or all of the views expressed are held by any individual author. In addition, the views expressed are those of the authors in their personal capacities and not in their official/professional capacities.
To cite this paper: James C. Cooper, et. al., “State Licensing Boards, Antitrust, and Innovation”, released by the Regulatory Transparency Project of the Federalist Society, November 13, 2017 (https://rtp.fedsoc.org/wp-content/uploads/RTP-Antitrust-Consumer-Protection-Working-Group-Paper-Occupational-Licensing.pdf).
Executive Summary
Every state has occupational licensing laws or regulations, which require individuals seeking to offer a certain service to the public first to obtain approval from the state. These laws and regulations raise numerous issues, including the economic freedom problems identified by the State and Local Working Group.1 This Paper focuses specifically upon the competitive implications of such regulations.
Occupational licensing requirements historically derive from a desire to protect unwitting consumers from bad actors. They were typically confined to professions where consumers struggled to ascertain the purported professional’s actual expertise and ability — and where the consumer’s misperceptions could have significant negative consequences. Thus, professions like medical and legal have long had self-imposed licensing regimes. The competitive concerns with occupational licensing generally do not arise at this fundamental level, when reasonable requirements directly tied to ensuring basic quality standards are established.
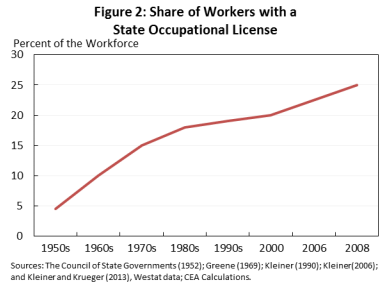
When, however, incumbents wield licensing requirements not as a defensive shield to protect consumers but as an offensive sword to exclude new entrants, serious concerns regarding the competitive implications of the licensing schemes arise. Self-interested incumbents have incentives that may differ from consumers, and these self-interested incumbents can — and sometimes do — impose requirements that do not enhance quality, but rather restrict output, increase prices, and hamper innovation. In other words, occupational licensing regimes can be contorted into schemes that exclude competitors and, in doing so, harm the very consumers they purport to protect. The likelihood of such abuses has increased tremendously in recent decades, as the number of licensed professions in the United States has skyrocketed:
2
Simultaneously, as new technologies and innovations have proliferated, these concerns have become increasingly pronounced.3 Today, incumbents relying upon older technologies frequently attempt to combat disruptive new entrants by imposing upon them licensing restrictions that are often outdated, irrelevant, or do not make sense to apply to the novel goods or services. For example, self-interested incumbents have established rules that would prevent the operation of innovative entrants and limit patients’ access to board-certified physicians in the state of Texas — a result particularly harmful in Texas, where there is a severe physician shortage.4
Given the proliferation of such undesirable results today, the U.S. Federal Trade Commission (FTC or Commission) recently established an Economic Liberty Task Force to further build upon the Commission’s longstanding, bipartisan work on occupational licensing and to discern additional ways to better protect consumers from harmful licensing requirements.5 Likewise, the U.S. Senate is considering a bill that would “combat the abuse of occupational licensing laws by economic incumbents.”6
This Paper explores the competitive implications of state occupational licensing regimes. Part I analyzes the historical development and justification for occupational licensing. Part II reviews the empirical evidence regarding the effects of occupational licensing on factors such as quality, price, innovation, and availability. Part III summarizes how antitrust law, and particularly the state action doctrine, treats state board-enacted occupational licensing. Part IV explores the interplay of occupational licensing and antitrust laws in the United States, delving into a particularly striking case at the intersection of occupational licensing and innovation: Teladoc, Inc. v. Texas Medical Board. Part V provides some suggestions for agency engagement in monitoring the effective use of occupational licensing.
I. The Anticompetitive Impetus for State Occupational Licensing Restrictions Today
Occupational licensing restrictions were traditionally enacted to protect consumers from unsavory fraudsters — think “quacks” with no medical training holding themselves out to be legitimate physicians, or similarly untrained individuals masquerading as lawyers. By establishing basic educational and training requirements, occupational licensing rules can accordingly serve very important functions.
The problem is that, today, occupational licensing requirements often fail to focus upon the goal of enhancing consumer outcomes and, instead, perversely seek to protect incumbents from competition. Consider, for instance, that the country has seen a dramatic increase in occupational licensing over the last several decades. Less than five percent of jobs in the American economy required a license in the 1950s. But today, economists estimate that between 25 and 30 percent of American occupations now require a license to operate.7
Exacerbating the sheer increase in scope is the problem of self-interested regulators. In many instances, the governing entity is not an independent group of elected officials directly accountable to the public, but rather a board of appointed practitioners whose primary job remains operating in the very same market they are regulating. Although licensing in some occupations may benefit the public by reducing information asymmetry and/or ensuring a minimum quality level for a particular service, the significant growth in the number of occupations governed by some form of licensing requirements, often enacted by self-interested incumbents, is a threat to consumer welfare.
Despite that many occupational licensing regimes harm consumers and tighten labor markets, such regimes appear to be growing ever more popular. One explanation for this conundrum — why are such bad laws so popular? — is that the beneficiaries of such laws have strong incentives to promote and maintain the laws’ existence. Public choice economics teaches that laws and regulations will be biased toward benefitting interest groups that are better organized and are likely to gain more from favorable rules, which increases such groups’ willingness to invest in acquiring political support.8 As one textbook explains, laws and regulations are “likely to benefit small interest groups with strongly held preferences at the cost of large interest groups with weakly felt preferences” — or in other words, a small group is able to extract concentrated benefits while dispersing the costs broadly.9 The individuals that benefit from strong occupational licensing restrictions — incumbent suppliers that already have a license — can benefit substantially from the high entry barriers afforded by occupational licensing and related restrictions. Moreover, this group is necessarily smaller than the harmed group, which not only includes putative workers in the licensed profession, but consumers as well. Consumers are the most worthwhile interest group, but often the most ignored.
Notwithstanding the harms to consumers that result from restricted entry, licensing boards typically justify such regulations by citing the need to protect the public from poor services due to asymmetric information. The typical argument goes something like this: because consumers cannot discern the quality of the service they are buying, there will be a “race to the bottom” in which only the worst quality providers survive absent a government-mandated quality floor. This is why licensing requirements have long existed where quality standards are deemed particularly important and the average consumer is likely to be at a severe information disadvantage relative to the provider (e.g., health care markets).
More recently, the same information problems have been put forward to justify restrictions on the use of technology by consumers to substitute for professional services (e.g., telemedicine, real estate, legal services). Of course these justifications have less purchase when applied to entry restrictions designed to hinder innovative rivals in the sharing economy (e.g., Uber, Lyft, Airbnb) — where one of the innovations rivals introduced was self-imposed fixes to such informational asymmetries (e.g., mandatory ratings and reviews of both the provider and the consumer). Accordingly, the relevant regulatory issue in such markets is whether to apply existing regulatory requirements designed to regulate traditional modes of services (e.g., taxis, hotels) to new forms of competition that use technology to address issues previously addressed through regulation.10
The obvious question these justifications raise is: does the implementation of licensing restrictions in fact enhance consumer outcomes?
Exacerbating the sheer increase in scope is the problem of self-interested regulators. In many instances, the governing entity is not an independent group of elected officials directly accountable to the public, but rather a board of appointed practitioners whose primary job remains operating in the very same market they are regulating.
II. The Consequences of Occupational Licensing: The Empirical Evidence
Economists and scholars have examined the empirical effects of occupational licensing in many contexts and forms.11 The competitive concerns with licensing mostly revolve around their potential negative effects upon both consumer and labor markets. An occupational licensing requirement is effectively a restriction on entry: it limits who can enter the market and under what circumstances. Licensing requirements may also restrict entry via related mechanisms such as commercial practice restrictions, ethics rules, restrictions on advertising, and scope of practice restrictions, which regulate the range of services a professional may offer.
Any government action that explicitly restricts the number of competitors that can enter a market, or otherwise raises the cost of entry by requiring entrants to have certain credentials or meet certain requirements, distorts market prices and output. Prices will be higher because sellers pass cost increases through to consumers.12 Output will be reduced because restrictions on, or higher costs of, entry result in fewer sellers operating in a given market.13 Absent some countervailing benefit, occupational licensing thus yields higher prices, reduced output, and lessened competition (competition which would, in turn, likely yield additional innovation and quality improvements).14 One study, in fact, estimates that occupational licensing restrictions cost about $203 billion per year.15
Occupational licensing also harms those seeking to practice the licensed occupation. These harms include time and money that would not be spent but for occupational licensing requirements, as well as fewer jobs. A typical occupational licensing restriction takes the form of requiring a potential licensee to have undergone a certain number of hours of education or to have achieved a particular degree, as well as paying a licensing fee (sometimes recurring) ostensibly to support the operations of the licensing board. For instance, one study examining low- and moderate-income licensed occupations found licensees were, on average, required to pay $209, pass an exam, and complete 275 days — or about nine months — of education and training.16 Many of these requirements vary significantly by state, which in effect taxes interstate movement by those who work in licensed professions, thereby negatively affecting the smooth operation of labor markets. Indeed, one study from 2011 estimates that occupational licensing restrictions have resulted in 2.85 million fewer jobs.17
At the same time, the purported benefits of occupational licensing requirements — particularly those imposed by active market participants — often fail to come to fruition in practice.18 This is not entirely surprising, given the disparity in licensed occupations among states. A 2015 White House report, for example, found that over 1,100 occupations are regulated in at least one state, but fewer than 60 are regulated in all 50 states.19 These numbers demonstrate that there exist “substantial differences” between what occupations states elect to regulate,20 thereby undermining the typical safety arguments associated with occupational licensing. That is, if licensing restrictions were truly required to protect consumers — or truly enhanced consumer outcomes — we would expect to see all the states regulating the same industries. But if only a handful of states require a license for, e.g., a locksmith or interior decorator, and the vast majority of states do not require such a license and are not experiencing poor consumer, then consumers are clearly not the primary beneficiaries of such laws. This is consistent with reports investigating occupational licensing, which have frequently found regulators behaving in ways that further their own ends, not consumers’.21
Indeed, numerous studies, covering a variety of occupations, concluded that licensing regulations and restrictions failed to increase quality — the purported rationale driving most licensing regimes.22 At the same time, the evidence shows that occupational licensing requirements consistently yield higher prices in the affected markets as well as increased wages for licensed professionals.23 These facts together — no quality improvements, higher prices, and higher wages — demonstrate quite clearly that quality-based arguments in favor of entry restrictions do not pass muster. Moreover, the case for prophylactic regulation that restricts entry as a means to ensure supplier quality is especially weak where modern technology — such as the reputation ratings systems developed by platforms operating in the sharing economy — provides tools that meaningfully reduce information asymmetries.
Meanwhile, there is evidence that relaxing entry restrictions can benefit consumers enormously.24 One working paper estimates that UberX service — which would be prohibited under a legacy taxi medallion licensing system — generated $6.8 billion in consumer surplus in the United States in 2015.25
How, then, to solve the pervasive and expensive problem of occupational licensing and entry restrictions? The simplest and best approach is for states to engage in smarter lawmaking and regulation by declining to adopt new licensing requirements and revising existing laws to reduce barriers to entry. The FTC’s Economic Liberty Task Force — which builds upon the Commission’s longstanding bipartisan tradition of monitoring and preventing this kind of abuse — and the proposed Senate legislation are each steps aimed in the direction of getting states to do just that. Eliminating or reducing existing licensing requirements for certain occupations is another approach. Yet another would be to reduce a state board’s ability to impact competition. For example, government certification could become one among many types of certification, rather than a necessary requirement to compete, and thus not act as an entry barrier. These strategies of reducing the pernicious effects of occupational licensure are not mutually exclusive.
We focus upon another important approach: using antitrust law to eliminate or invalidate specific activity by state boards. In this way, in addition to targeting specific examples of anticompetitive activity, antitrust can act as a catalyst to more wide-ranging reforms adopted through political processes.
Absent some countervailing benefit, occupational licensing thus yields higher prices, reduced output, and lessened competition (competition which would, in turn, likely yield additional innovation and quality improvements).14 One study, in fact, estimates that occupational licensing restrictions cost about $203 billion per year.15
III. The Role of Antitrust in Restraining Harmful Occupational Licensing Regimes
Regulation that restricts entry necessarily has anticompetitive effects and, as such, would presumptively be subject to federal antitrust laws. However, because most licensing regimes are enacted at the state level, the Supreme Court developed the “state action doctrine” to vindicate principles of federalism and to permit sovereign states deliberately to establish regulations that may negatively impact competition. In creating this doctrine, the Supreme Court reasoned that Congress did not intend the Sherman Act “to restrain a state or its officers or agents from activities directed by the legislature. In a dual system of government in which, under the Constitution, the states are sovereign, save only as Congress may constitutionally subtract from their authority, an expressed purpose to nullify a state’s control over its officers and agents is not likely to be attributed to Congress.”26 At the same time, the Court has repeatedly cautioned that “state-action immunity is disfavored, much as are repeals by implication.”27 Accordingly, the Supreme Court and the lower courts have developed limitations upon this doctrine intended to respect deliberate actions by state sovereigns, while preventing abuses of this limited immunity.
Some have characterized the Court’s creation of the state action doctrine as a continuation of its efforts to roll back Lochner era federal constitutional oversight of state economic policy.28 These authors argue further that the reasoning in Parker v. Brown does not — and should not — apply with equal force to the Federal Trade Commission Act, thus envisioning a larger and more active role for the Federal Trade Commission in prosecuting anticompetitive state regulations, including occupational licensing requirements and other restrictions on entry.29
Many cases since the Court first articulated the state action doctrine have clarified the conditions under which defendants can claim immunity from federal antitrust lawsuits. One important issue is whether a non-sovereign state actor can claim immunity. In California Retail Liquor Dealers Ass’n v. Midcal Aluminum, Inc.,30 the Supreme Court laid out a two-part test to determine if the State Action defense is available to non-sovereign actors: First, the party’s action must be pursuant to a “clearly articulated” and “affirmatively expressed” state policy to displace competition.31 Second, the state must actively review the party’s actions to assure that they comport with the state policy: “The supervisor must review the substance of the anticompetitive decision, not merely the procedures followed to produce it; the supervisor must have the power to veto or modify particular decisions to ensure they accord with state policy.”32
In FTC v. Phoebe Putney Health Sys., Inc.,33 the Supreme Court clarified what it means for a state to clearly articulate a state policy to displace competition. The conduct sought to be immunized must be a “foreseeable result” of the state policy, and there must be evidence that the state “affirmatively contemplated” that the substate actor “would displace competition” through its actions.34 It is not enough for a substate actor to point to “general powers routinely conferred by state law.”35
Municipalities, although not sovereign state actors, are subject only to the clear articulation prong.36 Private actors, however, are subject to both prongs of Midcal.37 Thus, if a state sets out a regulatory regime that relies on private market actors to engage in conduct that otherwise would violate the antitrust laws (e.g., jointly determine rates), the private actors only enjoy state action protection if their actions are both taken pursuant to a clearly articulated state policy to displace competition and supervised by the state.38 That is, the state must be sufficiently involved in the anticompetitive conduct to convert the otherwise private action into a politically accountable sovereign act.39
Before FTC v. North Carolina Dental State Bd. of Dental Examiners,40 it was unclear whether the antitrust laws would treat state boards more like municipalities, who need not be actively supervised by the state sovereign, or like private parties, who do. But in NC Dental, the Supreme Court cleared up this legal uncertainty. Analogizing them to private trade associations, the Court held both Midcal’s prongs apply to state boards controlled by market participants.41 It explained, “the need for supervision turns not on the formal designation given by the states to their regulators, but on the risks that active market participants will pursue private interest in restraining trade.”42
Accordingly, the Supreme Court has devoted considerable thought to crafting its law and doctrine in a way that allows antitrust to remain a key tool in the arsenal for combating abusive occupational restraints. The relevance — and importance — of these doctrines is on display in several key litigations affecting a range of occupations today.43 Below, we focus upon the striking case of Teladoc, Inc. v. Texas Medical Board.
Analogizing them to private trade associations, the Court held both Midcal’s prongs apply to state boards controlled by market participants.41 It explained, “the need for supervision turns not on the formal designation given by the states to their regulators, but on the risks that active market participants will pursue private interest in restraining trade.”42
Receive more great content like this
IV. The Occupational Licensing, Antitrust, and the State Action Doctrine in Innovative Markets: Teladoc, Inc. v. Texas Medical Board
Occupational licensing regimes are particularly prone to misuse in innovative markets. When disruptive new entrants threaten to upset the foundational workings of a market with strong incumbents, those incumbents are likely to react by erecting rules and regulations to preserve the status quo. Numerous examples have made their way into the popular media (and the courts), including the troubles companies like Uber and Lyft have had with traditional taxis regimes, and companies like AirBnB have had with hotels.44
The case of Teladoc Inc. v. Texas Medical Board45 presents a particularly germane example of incumbents enacting rules that thwart entry and threaten consumers. In that case, the Texas Medical Board (TMB), comprised mostly of active physicians, enacted a rule that would limit patients’ ability to obtain cheaper, more accessible medical care from Teladoc physicians. Plaintiff Teladoc employed “board certified physicians who are provided specialized training in treatment and diagnosis via telephone,” to offer certain services to patients (typically those whose insurance provider contracted with Teladoc).46 Teladoc physicians would accept a request for consultation, review the requesting patient’s information and medical records (via Teladoc’s website), and then call the patient.47 Based upon this background information and the additional information the physician elicited during the call with the patient, the physician would then offer medical advice, including referring the patient to a doctor’s or dentist’s office or emergency room.48 Teladoc physicians were also permitted to prescribe certain medications.49
TMB revised its rules in 2015 to require a “face-to-face visit or in-person evaluation” before a physician could issue any prescription.50 Teladoc challenged this revision as a violation of federal antitrust laws, the effects of which would be to increase prices, reduce choice, reduce access, reduce innovation, and reduce the overall supply of physician services.51
As to state action immunity, both parties stipulated that active supervision was required under NC Dental.52 TMB proffered several means of supervision to which it was subject, including judicial review of TMB decisions by the courts of Texas, the State Office of Administrative Hearings, and the Texas Legislature.53 The court, however, found the review these forums provided was “limited and fail[ed] to confer on the reviewing court a method for looking to whether the decision of the TMB is ‘in accord with state policy.’”54 It further noted that the reviewing court had no authority to modify any TMB decision, but only to reverse or remand, and that case law consistently rejected that such review could constitute active supervision.55 The court’s decision thus prevented a self-interested board acting largely free from state oversight from invoking antitrust immunity.
On the merits, this case of incumbent abuse was particularly egregious: It would deliberately curtail patients’ access to board-certified physicians (who were often working with the patient’s insurance company). This rule would be especially harmful in Texas, which suffers from a staggering shortage of doctors. Texas ranks 41st nationally in physicians per capita, and 47th in primary care physicians per capita.56 In fact, one report estimated that it would require nearly 13,000 additional physicians just to bring Texas up to the national average.57 And even these staggering numbers understate the problem of healthcare access, as patients in remote areas would likely remain isolated even with a massive influx of physicians to the state.58 Accordingly, the self-interested board was restricting entry of certified physicians just where their services were needed most.
The FTC has, in fact, recognized that the competitive effects of such regulations may be “especially striking where there are primary care shortages, as in medically underserved areas or with medically underserved populations” — just the conditions that exist in Texas.59 Indeed, at the time this case arose, the FTC had already extensively examined similar scope of practice rules in healthcare markets — and consistently concluded that such rules typically do more harm than good.60 In this specific case, Teladoc presented consistent, striking evidence that TMB’s new rule would inflict significant consumer harm. Teladoc, for instance, proffered evidence that the average costs of a visit to a physician’s office or emergency room (two close substitutes to calling a Teladoc physician) were $145 and $1,957, respectively, while the cost of a Teladoc consultation averaged just $40.61
TMB’s new rule would, accordingly, have imposed very real costs upon patients in Texas, negatively affecting the provision of healthcare in the state. Indeed, Teladoc presents a compelling example of incumbents perverting occupational licensing regimes to exclude board-certified entrants, to reduce patients’ access to those qualified entrants, and to raise prices to patients. Simultaneously, this case demonstrates how antitrust laws can successfully intervene to protect consumers from such abuses and to halt these harmful effects. The utility of antitrust — and the commensurate benefits to consumer welfare from antitrust engagement — is on full display here. The antitrust laws played a key role in preventing very harmful effects from being realized in Teladoc, and can do so in many other settings, as well. As such, we offer some recommendations for directing antitrust engagement below.
Indeed, Teladocpresents a compelling example of incumbents perverting occupational licensing regimes to exclude board-certified entrants, to reduce patients’ access to those qualified entrants, and to raise prices to patients. Simultaneously, this case demonstrates how antitrust laws can successfully intervene to protect consumers from such abuses and to halt these harmful effects
V. Areas of Engagement
Occupational licensing reform currently enjoys wide bipartisan support. For example, the FTC has a long history — across Republican and Democratic administrations — of competition advocacy and enforcement actions aimed at state and local restraints on competition. The focus of these advocacy efforts has been to articulate the harm to consumers that can result from actions by public actors that restrict the number of suppliers or raise the cost of entering a particular market. In addition, a report from the Obama administration’s Council of Economic Advisors in the summer of 2015 described the effect licensing restrictions have on labor markets. The report provided evidence that occupational licensing requirements create income inequality — licensed professionals earn more than non-licensed professionals even when controlling for education and other factors. What is more, in the wake of NC Dental, states are looking for guidance.
The FTC has a number of tools available to reduce the economic harm caused by occupational licensing and other state restrictions on entry:
- Competition advocacy: the FTC should continue to advocate pro-competition policy. Since at least the early 1980s, the FTC has submitted letters to state and local regulators explaining the cost to consumers associated with occupational licensing and other similar restrictions. The success of these efforts in any individual instance is dependent upon a number of factors, but in general the competition advocacy program enjoys broad bi-partisan support from FTC commissioners and continues apace with each new administration. The Commission should increase its efforts in this area, and Acting Chairman Ohlhausen’s newly announced Economic Liberty Task Force is a good sign.
- Litigation: the FTC should continue to bring enforcement actions challenging anticompetitive restraints adopted by substate entities, such as its case against the North Carolina Board of Dentistry. Moreover, it can participate as an amicus in similar antitrust actions brought by private parties.
- Narrowing the reach of Parker v. Brown: The FTC can take steps to narrow the reach of Parker v. Brown and/or advocate that the Supreme Court overturn or limit the reach of the decision.
- One approach is for the FTC to work within the broader framework established by Parker v. Brown to narrow the sphere of immunity conferred by the two-part test established in Midcal. The FTC’s enforcement actions in Phoebe Putney and NC Dental can be seen as efforts by the Commission to narrow the scope of the clear articulation and active supervision requirements, making it relatively more difficult for states to establish that state law clearly articulates a purpose of displacing competition and/or that a substate entity is actively supervised by a sovereign state actor. Continuing down this path would — potentially — be an effort by the FTC to argue that the Supreme Court should reverse Town of Hallie and hold that municipalities must be actively supervised by a sovereign state actor when engaging in activity that would otherwise violate the Sherman Act.
- A different and more aggressive approach would be for the FTC to argue that Parker v. Brown does not control actions brought by the FTC under its authority to prosecute unfair methods of competition pursuant to Section 5 of the FTC Act. Because the FTC alone has the authority to enforce Section 5, any concern about an explosion in the number of antitrust actions challenging state and local laws would be muted. Moreover, by following this approach, the FTC could shed light directly on the anticompetitive effects of occupational licensing and other restrictions on entry, rather than focusing its efforts on shaping the legal doctrine established by Parker v. Brown.
- In addition, private litigants and other interest groups can use the antitrust laws to challenge anticompetitive state action. An example of this approach is the Chamber of Commerce’s lawsuit seeking to enjoin a Seattle city law allowing drivers for ride-sharing companies like Uber and Lyft to bargain collectively with the platforms.
Footnotes
1 Dana Berliner, et. al., Occupational Licensing Run Wild, Reg. Transparency Project of the Federalist Soc’y, 23 (Nov. 7, 2017), https://rtp.fedsoc.org/wp-content/uploads/RTP-State-Local-Working-Group-Paper-Occupational-Licensing.pdf. The State and Local Working Group demonstrated human (non-economic) costs, presenting several stories of ordinary individuals harmed by state licensing laws. Id. In one example, a woman (who was a cancer survivor herself) built a business that arranged for licensed cosmologists to conduct home visits for cancer patients too sick to travel. However, she was forced to endure sixteen months of litigation when the Arizona Board of Cosmetology required that she be licensed even though she neither cut hair nor operated a salon. Id. at 25. These narratives, and the human costs they illustrate, are an important part of the larger discussion on state licensing regimes.
2 See U.S. Dep’t of Treasury, Office of Econ. Pol’y, Council of Econ. Advisors, & Dep’t of Labor, Occupational Licensing: A Framework for Policymakers, at 5 (2015), https://obamawhitehouse.archives.gov/sites/default/files/docs/licensing_report_final_nonembargo.pdf [hereinafter White House Report].
3 See, e.g., Joshua D. Wright, Comm’r, U.S. Fed. Trade Comm’n, Regulation in High-Tech Markets: Public Choice, Regulatory Capture, and the FTC, Remarks at the Big Ideas about Information Lecture, Clemson University, Clemson, South Carolina (Apr. 2, 2015), https://www.ftc.gov/system/files/documents/public_statements/634631/150402clemson.pdf
4 See infra Section IV, discussing Teladoc Inc. v. Tex. Med. Bd., 112 F. Supp. 3d 529 (W.D. Tex. 2015).
5 U.S. Fed. Trade Comm’n, Economic Liberty, https://www.ftc.gov/policy/advocacy/economic-liberty (last visited Oct. 29, 2017). The FTC has a history of investigating and reporting upon the effects of occupational licensing. See, e.g., Wright, supra note 3, at 15-18 (summarizing the FTC’s engagement with occupational licensing issues from the 1970s onwards); U.S. Fed. Trade Comm’n, Competition and the Regulation of Advanced Practice Nurses (2014), https://www.ftc.gov/reports/policy-perspectives-competition-regulation-advanced-practice-nurses [hereinafter FTC APRN Report]; U.S. Fed. Trade Comm’n & Dep’t of Justice, Improving Health Care: A Dose of Competition, ch. 2, at 25-33 (2004), http://www.ftc.gov/reports/healthcare/040723healthcarerpt.pdf
6 Proposed Legislation, Restoring Board Immunity Act of 2017 (RBI Act), S. 1649, 115th Cong. 1st Session, https://www.congress.gov/bill/115th-congress/senate-bill/1649/text
7 See White House Report, supra note 2, at 5 (“More than one-quarter of U.S. workers now require a license to do their jobs, with most of these workers licensed by the States. The share of workers licensed at the State level has risen five-fold since the 1950s.”); Press Release, U.S. Fed. Trade Comm’n, FTC Announces Second Economic Liberty Public Roundtable (Sept. 11, 2017), https://www.ftc.gov/news-events/press-releases/2017/09/ftc-announces-second-economic-liberty-public-roundtable (“Nearly 30 percent of U.S. jobs require a license today, up from less than five percent in the 1950s.”).
8 See, e.g., Milton Friedman, Capitalism and Freedom 142-43 (U. Chi. Press, 1962); Research Reports, Occupational Licensure Laws: A Review of Some Findings, 8 Am. Inst. Econ. Research 71, 72, https://www.aier.org/sites/default/files/Files/Documents/Research/899/RR199015.pdf (“The pressure to regulate occupations historically has come from the groups that stand to lose from competition. Occupational licensure laws raise barriers to entry and prevent many otherwise qualified individuals from entering the trade or profession.”); George J. Stigler, The Theory of Economic Regulation, 2 J. Econ. & Mgmt. Sci. 3, 13-14 (1971); Gordon Tullock, The Welfare Costs of Tariffs, Monopolies and Theft, 5 W. Econ. J. 224 (1967); Amy Humphris, Morris M. Kleiner, & Maria Koumenta, How Does Government Regulate Occupations in the UK and US? Issues and Policy Implications, in Labour Market Policy for the 21st Century (Oxford U. Press, 2010), http://lgi.umn.edu/centers/freeman/pdf/Kleinerpaper.pdf
9 W. Kip Viscusi et al., Economics of Regulation and Antitrust 382 (4th ed. 2005).
10 Wright, supra note 3, at 14 (“In my view . . . there ought to be a general skepticism of all regulation of technologies and business models that threaten to disrupt an industry. Indeed, hearing a regulator say something like ‘we need to watch closely because Company X may disrupt the industry’ is in effect an admission by the regulator that whatever regulation he is about to adopt is one that will harm consumers.”).
11 Morris M. Kleiner, Occupational Licensing, 14 J. Econ. Persp. 189, 189 (2000) (“The study of the regulation of occupations has a long and distinguished tradition in economics.”).
12 See Sidney L. Carroll & Robert J. Gaston, Occupational Licensing and the Quality of Service: An Overview, 7 L. & Human Behavior 139, 140 & n.3 (1983) (“[L]icensing has been shown repeatedly to have an upward price effect.”).
13 See, e.g., Morris Kleiner, Alan Krueger & Alexandre Mas, A Proposal to Encourage States to Rationalize Occupational Licensing Practices, at 1 (2011), https://www.hhh.umn.edu/file/9441/download (“It is well understood that occupational licensing can serve as a barrier to occupational entry resulting in reduced employment, monopoly rents for workers in the occupation, and higher prices for consumers.”); Eugene R. Declercq et al., State Regulation, Payment Policies, and Nurse-Midwife Services, 17 Health Affairs 190 (1998) (finding rules “supportive” of nurse midwife practice associated with increased distribution of nurse midwives and their services); Edward S. Sekscenski et al., State Practice Environments and the Supply of Physician Assistants, Nurse Practitioners, and Certified Nurse-Midwives, 331 N. Engl. J. Med. 1266 (1994) (finding stringent restrictions upon nurse practitioners and specialized advanced practice registered nurses are associated with fewer per capita practitioners).
14 Carolyn Cox & Susan Foster, Staff Report Bureau of Econ., Fed. Trade Comm’n, The Costs and Benefits of Occupational Regulation, at v (1990), http://www.ramblemuse.com/articles/cox_foster.pdf (“This report finds . . . that occupational licensing frequently increases prices and imposes substantial costs on consumers. At the same time, many occupational licensing restrictions do not appear to realize the goal of increasing the quality of professionals’ services.”).
15 Morris Kleiner, Alan Krueger & Alexandre Mas, A Proposal to Encourage States to Rationalize Occupational Licensing Practices, at 3 (2011), https://www.hhh.umn.edu/file/9441/download; see also Morris M. Kleiner, Reforming Occupational Licensing Policies (The Hamilton Project, Discussion Paper 2015-01, Mar. 2015), https://www.brookings.edu/wp-content/uploads/2016/06/THP_KleinerDiscPaper_final.pdf
16 Dick M. Carpenter, II, Lisa Knepper, Angela C. Erickson & John K. Ross, License to Work: A National Study of Burdens from Occupational Licensing, at 14 (2012), http://ij.org/wp-content/uploads/2015/04/licensetowork1.pdf
17 Kleiner et al., supra note 13, at 3.
18 See, e.g., FTC APRN Report, supra note 5, at 39 (“When faced with proposals to narrow APRN scope of practice . . . legislators are encouraged to apply a competition-based analytical framework and carefully scrutinize purported health and safety justifications. In many instances, legislators may well discover that there is little or no substantiation for claims of patient harm.”).
19 White House Report, supra note 2, at 4.
20 Id.
21 See, e.g., Cox & Foster, supra note 14, at v (“[T]he majority of the evidence indicates that licensing proposals are often not in the consumers’ best interest.”); Humphris et al., supra note 8, at 15 (“Governments and regulatory bodies are advised to carefully scrutinize any proposals for occupational licensing given that the evidence demonstrates the existence of a strong element of self-interest behind requests to be licensed.”); FTC APRN Report, supra note 5, at 15 (“It may be in the economic self-interest of those physicians [on the board] to propose and advocate the adoption of restrictions on [Advanced Practice registered Nurses] licensure and scope of practice; and such physicians might be biased towards doing so.”).
22 See, e.g., Cox & Foster, supra note 14, at v (“[M]any occupational licensing restrictions do not appear to realize the goal of increasing the quality of professionals’ services.”); FTC APRN Report, supra note 5, at 36-37 (“Specifically, our research did not identify significant evidentiary support for either the claim that independent APRN practice gives rise to significant safety concerns, or the claim that mandatory supervision requirements redress such concerns. . . . [W]e have not seen research suggesting that the safety or quality of primary care services declines when APRN supervision or collaborative practice requirements are lessened or eliminated.”); White House Report, supra note 2, at 4 (“[I]n a number of other studies, licensing did not increase the quality of goods and services, suggesting that consumers are sometimes paying higher prices without getting improved goods or services.”); Morris M. Kleiner & Robert T. Kudrle, Does Regulation Affect Economic Outcomes? The Case of Dentistry, 43 J.L. & Econ. 547, 575-76 (2000) (finding that “tougher licensing does not improve outcomes, but it does raise prices for consumers and the earnings of practitioners”).
These results hold when examining the effects of occupational regulations such as advertising restrictions. See, e.g., Timothy Muris, California Dental Association v. Federal Trade Commission: The Revenge of Footnote 17, 8 Sup. Ct. Econ. Rev., at 293-304 (surveying numerous studies testing the price and quality effects of advertising); R.S. Bond, J.J. Kwoka, J.J. Phelan, & I.T. Whitten, FTC Bureau of Economics Staff Report, Effects of Restrictions on Advertising and Commercial Practice in the Professions: The Case of Optometry, (1980), https://www.ftc.gov/sites/default/files/documents/reports/effects-restrictions-advertising-and-commercial-practice-professions-case-optometry/198009optometry.pdf (“The data in this study support the view that advertising and commercial practice lower prices. . . . The data are not consistent with the view that advertising and commercial practice lower the quality of professional care available in the market.”); John E. Kwoka, Jr., Advertising and the Price and Quality of Optometric Services, Amer. Econ. Rev., Vol. 74, No. 1 (March 1984), pp. 211-16 (concluding that “considerable social benefits” may derive from relaxing advertising restrictions); Timothy J. Muris & Fred S. McChesney, Advertising and the Price and Quality of Legal Services: The Case for Legal Clinics, Amer. Bar Found. Research J., Vol. 4, No. 1 (Winter 1979), pp. 179-207 (concluding that advertising for legal services led to decreases in prices with no diminishment in quality); Lee Benham, The Effect of Advertising on the Price of Eyeglasses, J.L & Econ., Vol. 15, No. 2, pp. 337-52 (finding that optometrist prices in U.S. states that prohibited advertising were twenty-five percent higher than in states without such prohibitions); Deborah Haas-Wilson & Elizabeth Savoca, “Quality and Provider Choice: A Mutlinomial Logit-Least-Squares Model with Selectivity”, Health Serv. Research, Vol. 24, No. 6 (February 1990), pp. 791-809 (“Proponents of regulations restricting the commercial practices of optometrists argue that the regulations are necessary to prevent adverse health outcomes and to protect consumers from low-quality vision care. Our results suggest, however, that such restrictions are failing to improve health outcomes in the contact lens industry and may even be lowering them.”).
23 See, e.g., White House Report, supra note 2, at 56 (“[T]he practice of licensing can impose substantial costs on job seekers, consumers, and the economy more generally.”); id. at 4 (“Estimates find that unlicensed workers earn 10 to 15 percent lower wages than licensed workers with similar levels of education, training, and experience. Licensing laws also lead to higher prices for goods and services, with research showing effects on prices of between 3 and 16 percent.”).
24 See, e.g., Lee Benham, The Effect of Advertising on the Price of Eyeglasses, J.L. & Econ., Vol. 15, No. 2, pp. 337-52 (finding that optometrist prices in U.S. states that prohibited advertising were twenty-five percent higher than in states without such prohibitions); John E. Kwoka, Jr., Advertising and the Price and Quality of Optometric Services, Amer. Econ. Rev., Vol. 74, No. 1 (March 1984), pp. 211-16 (concluding that “considerable social benefits” may derive from relaxing advertising restrictions); Timothy J. Muris & Fred S. McChesney, Advertising and the Price and Quality of Legal Services: The Case for Legal Clinics, Amer. Bar Found. Research J., Vol. 4, No. 1 (Winter 1979), pp. 179-207 (concluding that advertising for legal services led to decreases in prices with no diminishment in quality).
25 Peter Cohen, et. al., Using Big Data to Estimate Consumer Surplus: The Case of Uber (NBER Working Paper No. 22627, Sept. 2016), http://www.nber.org/papers/w22627; see also Nicholas Buchholz, Spatial Equilibrium, Search Frictions and Efficient Regulation in the Taxi Industry (Oct. 26, 2017), https://scholar.princeton.edu/sites/default/files/nbuchholz/files/taxi_draft.pdf
26 Parker v. Brown, 317 U.S. 307, 313 (1943).
27 FTC v. Phoebe Putney Health Sys., Inc., 568 U.S. 216, 225 (2013) (quoting FTC v. Ticor Title Ins. Co., 504 U.S. 621, 636 (1992)).
28 Daniel A. Crane & Adam Hester, State-Action Immunity and Section 5 of the FTC Act, 115 Mich L Rev. 365, 367-68 (2016); Merrick B. Garland, Antitrust and State Action: Economic Efficiency and the Political Process, 96 Yale L.J. 486, 487-88 (1987).
29 Crane & Hester, supra note 28, at 368-369.
30 Cal. Retail Liquor Dealers Ass’n. v. Midcal Aluminum, Inc., 445 U.S. 97 (1980).
31 Id. at 105.
32 N.C. State Bd. of Dental Exam’rs v. FTC, 135 S.Ct. 1101, 1116 (2015).
33 FTC v. Phoebe Putney Health Sys., Inc., 568 U.S. 216, 225 (2013).
34 Id. at 228-30.
35 Id. at 227-28.
36 Hallie v. Eau Claire, 471 U.S. 34, 46 (1985).
37 N.C. Dental, 135 S.Ct. at 1111-12, 1114 (holding market participants serving on a state dental board qualified as private actors for state action purposes); S. Motor Carriers Rate Conf. v. United States, 471 U.S. 48, 56 (1985).
38 See S. Motor, 471 U.S. at 62.
39 See N.C. Dental, 135 S.Ct. at 1111; FTC v. Ticor Title Ins. Co., 504 U.S. 621, 636 (1992).
40 135 S.Ct. 1101.
41 Id. at 1114 (“[A] state board on which a controlling number of decision makers are active market participants in the occupation the board regulates must satisfy Midcal’s active supervision requirement in order to invoke state-action antitrust immunity.”).
42 Id.
43 Clark v. Seattle, No. C17-0382RSL (W.D. Wash. Aug. 24, 2017), on appeal, No. 17-35693 (9th Cir.); Wallen v. St. Louis Taxicab Comm’n, No. 4:15-cv-1432 HEA, 2016 WL 5846825, (E.D. Mo. Oct. 6, 2016); U.S. Chamber of Commerce v. Seattle, No. 2:16-CV-00322, 2016 WL 836320 (W.D. Wash. Mar. 3, 2016) on appeal, No. 17-35371 (9th Cir.); Teladoc, Inc. v. Tex. Med. Bd., 112 F. Supp. 3d 529 (W.D. Tex. 2015).
44 Wallen, 2016 WL 5846825; Wright, supra note 3, at 4.
45 Teladoc Inc. v. Tex. Med. Bd., 112 F. Supp. 3d 529 (W.D. Tex. 2015).
46 Id. at 533.
47 Id.
48 Id.
49 Id. The court noted Teladoc stated its physicians did not prescribe “DEA-controlled substances (including narcotics) or what are referred to as lifestyle drugs (i.e., Viagra, or diet pills).” Id. at 533, n.2.
50 Teladoc, 112 F. Supp. 3d at 534. In 2011, TMB issued a letter to Teladoc, stating that its rules (particularly 22 Tex. Admin. Code § 190.8) required a “face-to-face” examination before prescribing a dangerous drug or controlled substance. Id. The letter clearly conveyed TMB’s position that Teladoc and its physicians were violating the rule by issuing prescriptions following telephone conversations. Id. Teladoc challenged TMB’s interpretation, and the Texas Court of Appeals held the letter’s interpretation procedurally invalid, finding “TMB’s pronouncements in its June 2011 letter are tantamount to amendments to the existing text,” which listed a “face-to-face” examination as a possible — but not required — method for establishing a proper physician-patient relationship. Id. (citing Teladoc, Inc. v. Tex. Med. Bd., 453 S.W.3d 606, 620 (Tex. App. Austin 2014, pet. filed)). In response, TMB issued an “emergency” rule on January 16, 2015, amending the old Rule 190.8. Id. Teladoc sought and obtained a temporary injunction of the emergency rule in Texas state court. Id. TMB then conducted formal rulemaking, and the new rule passed vote on April 10, 2015.
51 Teladoc, 112 F. Supp. 3d at 537.
52 Teladoc, Inc. v. Tex. Med. Bd., No. 1-15-CV-343, 2015 WL 8773509, at *7 (Dec. 14, 2015) (holding TMB failed to meet its burden to prove state action immunity because it failed to show active supervision, and not reaching the question of clear articulation).
53 Teladoc, No. 1-15-CV-343, 2015 WL 8773509, at *7-10.
54 Teladoc, No. 1-15-CV-343, 2015 WL 8773509, at *9.
55 Teladoc, No. 1-15-CV-343, 2015 WL 8773509, at *9 (citing Patrick v. Burget, 486 U.S. 94, 104-05 (1997) (holding review process limited to discerning whether the board followed “some sort of reasonable procedure” and “there was evidence from which it could be found that plaintiff’s conduct posed a threat to patient care,” fell “far short of satisfying the active supervision requirement” (internal citations omitted)); Pinhas v. Summit Health, Ltd., 894 F.2d 1024, 1030 (9th Cir. 1989) (holding no active supervision when judicial review was limited to ascertaining whether “the decision was substantively rational, lawful, not contrary to established public policy and the proceedings were fair,” when the “court may not substitute a judgment of that of the governing board even if it disagrees with the board’s decision”); Shahawy v. Harrison, 875 F.2d 1529, 1535-36 (11th Cir. 1989) (finding no active supervision when “courts merely review the board’s decisions for procedural error and insufficient evidence”).
56 N. Tex. Regional Extension Ctr., The Physician Workforce in Texas, at 3 (2015), http://www.merritthawkins.com/UploadedFiles/MerrittHawkings/Surveys/Merritt_Hawkins_NTREC_Physician_Workforce_Survey.pdf
57 Id.
58 Id.
59 See, e.g., FTC APRN Report, supra note 5, at 4; see also id. at 21 (“Rural communities, too, are particularly vulnerable to provider shortages and access problems.”).
60 See, e.g., FTC APRN Report, supra note 5; see also Comment from FTC Staff to the Hon. Theresa W. Conroy, Conn. House of Representatives (Mar. 19, 2013), http://www.ftc.gov/os/2013/03/130319aprnconroy.pdf; Comment from FTC Staff to the Hon. Thomas P. Willmott & Hon. Patrick C. Williams, La. House of Representatives (Apr. 20, 2012), http://www.ftc.gov/os/2012/04/120425louisianastaffcomment.pdf; Comment from FTC Staff to the Hon. Paul Hornback, Commonwealth of Ky. State Senate (Mar. 26, 2012), http://www.ftc.gov/os/2012/03/120326ky_staffletter.pdf; Comment from FTC Staff to the Hon. Rodney Ellis & Hon. Royce West, Senate of the State of Tex. (May 11, 2011), http://www.ftc.gov/os/2011/05/V110007texasaprn.pdf; FTC Staff Comment Before the Mass. House of Representatives Regarding House Bill 2009 Concerning Supervisory Requirements for Nurse Practitioners and Nurse Anesthetists (Jan. 17, 2014), https://www.ftc.gov/sites/default/files/documents/advocacy_documents/ftc-staff-comment-massachusetts-house-representatives-regarding-house-bill-6-h.2009-concerning-supervisory-requirements-nurse-practitioners-nurse-anesthetists/140123massachusettnursesletter.pdf; Written Testimony from FTC Staff to Subcomm. A of the Joint Comm. on Health of the State of W. Va. Legislature (Sept. 10-12, 2012), http://www.ftc.gov/os/2012/09/120907wvatestimony.pdf
61 Teladoc Inc. v. Tex. Med. Bd., 112 F. Supp. 3d 537 (W.D. Tex. 2015).